 News
News  Market Data
Market Data  Discover
Discover 
Support: 888-992-3836
Copyright © 2023 InvestorsHub Inc.





Register for free to join our community of investors and share your ideas. You will also get access to streaming quotes, interactive charts, trades, portfolio, live options flow and more tools.
25$ per share with current fully diluted 1.7b share authorized? And soon to be 2b plus (and yes it is coming). Think about market cap in this abnormally large share count.....$25 will never happen. Please stop promoting this kind of BS. This stock will never even see double digits in your lifetime.
Yeah exactly you get an pdufa and/or an adcom date with the fda and similar with ema. You can use vertex as a guide as to how long it would take in the UK. They submitted in dec and got approved in November and that was without an RFI. You can be rest assured NWBO will get an RFi since they can't do anything right. So that's how you can deduct 2025 for the UK decision.
Sharpie, This is very encouraging. Thanks for sharing!!!
NWBO apparently told you recently that they are working their
tail off and we are only 128 days past MAA submission. So that
doesn't tell us anything about whether or not they will receive
approval within the 150 day target or whether they will have
to continue working their tail off for 60 or many more days
thereafter.
No one knows on this board when where or how. Everyone guessing or dropping names. It's funny I am clueless on this subject but not one guess by anyone has been close. That's like throwing 1000 dart and never even hitting the stupid board. Only ones that are right are the fudsters, look at the price. 120 days then 150 days now 150 days plus 60 days . Bunch of nostradomus not.
Thank you Bright Boy but my calculation for a 150
days+60 days RFI puts us at approval no later than
August 1 and if all the RFI issues are resolved
prior to the 60 day RFI extension, we may received an
even earlier MHRA decision.
So approval by let's say on September 30 would be about 270
days from acceptance of the MAA and would be approximately
equal to the time it took for the MHRA to reach a decision concerning
88% of the MAAs before the introduction of their 150 day accelerated
review program.
That does not sound like the 150 day fast track program initiated
for 2024 and a September 30 approval or disapproval decision
would suggest to me that NWBO's application for the 150 day
program was not accepted or that MHRA has not yet succeeded to
properly implement their accelerated MAA review.
I hope of course that I am wrong and that we will receive an approval decision
well before 9/30/24.
You talked to the company and they said they are currently working their tails off?
….And I think it could easily happen sooner, for reasons you are familiar with. 
Just to be clear, you're talking about MHRA acceptance of the SAP for PIP and not the Plll trial?
>>and formally announced acceptance of the SAP
From all my buds in London, the MHRA does not tell any company anything about dates AND they are telling me that it's the 150 plus 60. No if, ands or buts!!! So everyone needs to take a deep breath and look an approval mid to late third quarter and for RFI, the company and the MHRA are doing that every day!!!
Cheers,
BB
“ Theoretically, if no RFI is required, the application could be decided on within 150 days. “
If you talk with anyone from the company, you will learn they all are working their tails off to get it approved.
This means they got a RFI. Besides, it is unreasonable to think that with a 1.7m page submittal, the MHRA wouldn’t have any questions.
It is best to assume near worse case and that is a 210 day process. Anything less than 210 would be fantastic.
That may very will be so. I’ve been long 13+ years, so I’m hardened to all this. But, i wonder what you guess the pps will do in the interim?
Exactly. And historically it takes a little longer than that. So August to September! Just my guess.
We won't know if a RFI has been or will be issued.
space-farm - The corporation controlled healthcare system is training more and more morons with medical degrees, who have forgotten the art of critical thinking. I don't believe additional cell therapies would necessarily overrun DCVAX, on the contrary, these clock punchers aren't as interested as you might think, to keep all those options in their heads, let alone motivate themselves to learn how they work, and when to apply them. At least with DCVAX, physicians won't have any worries explaining toxicity complications. When the treatment is worse than the disease.
sharpie510,
“Starting in 2025…”, cryo storage prominent at the end of the presentation. Not sure the cryo storage is needed for the other prospects listed in the 2023 piece. Definitely needed for DCVax-L and they have plenty of it; ). Seems like 2025 and the word “cure(s)” are cornerstones for this new division. Best wishes.
That didn't take long at all. LOL. Back to Colonel Klink.
Yesterday:
"I'm tired of this bleeding day by day, also tired of this silence and this disrespectful management. No ASM, no quarterly calls, no adequate communication, no clarity, supposed hidden reasons for a quiet periods, copy-paste answers from DI, supposed hidden reasons for a quiet periods, etc. This is not the way to run a public company. "
Today:
"That is my idea, to buy again at least the number of shares I sold and maybe more as you mentioned."
Can't make it up.
learningcurve2020,
Don’t worry about NWBO as they have had extensive talks with MHRA over the years and formally announced acceptance of the SAP which in those talks also would have included the rational for changes in primary objectives/endpoints which is why the PIP was accepted. Try another more believable distraction next time ; ). Best wishes.
Thanks a lot manibiotech for your words and support. That is my idea, to buy again at least the number of shares I sold and maybe more as you mentioned.
Wow,,,,,$25 is amazing for all investors. Thank you. Hope your hunch is right.
Maybe best post of the day. You see what they do. Just like that they're all shifting to the end of summer. That's how it always works here, dragging it on and on, year after year after year. The MHRA approval process is much murkier than the FDA and EMA, who actually provide a target action date. Probably the reason LP submitted to MHRA. With the help of the disciples here she could easily drag this out until next year.
One guess is that there are a lot of politicians getting their palms greased in one way or another, who are beholding, and “enforcement types” who might not be eager to possibly “hurt” their careers and make big trouble for the “golden geese.”
What, you have a hard time believing that money and influence talks? (Thickly sarcastic comment in case you couldn’t tell)
Yes agree the competition & money never sleeps… but I really believe your patience and our investment will payoff handsomely! I also feel - take it for what it’s worth - that there will be a strong emotional play with NWBO. Once MHRA approves, Nature publication etc, this SP will move fast. And it’s my opinion that using the new pathway with England, Australia etc, sorry forgot exact name, that FDA approval is in play just before the election! GLTU
But then there is the thing called - how much time has MHRA actually taken on average to approve the applications submitted under 150 day path. And then there is assumption that MHRA actually agreed to consider it under 150 day path .
Respectfully, why the DOJ don’t intervene?
But I have read so many longs here in this board said they expected no RFI during the past. Did they all read it wrong? In US, a lot of fast track drug only needs 6 months to get approval, normal track needs 10 months. NWBO needs to wait that long to have dcvax-l to get approval?
Sorry you can’t comprehend how allowing patients to out live a death sentence is a positive thing.
I understand the financial constraints and respect your point and to be completely fair the cell therapy landscape has changed so much since this company started. I think it’s more wishful thinking because there are a lot of early stage companies with promising technology that have obtained very strong business development relationships for funding. look at Arcellx and Gilead.
I understand the frustration as you’ve been invested longer than I, but the “intelligent enough” bs is lazy… they needed to make fiscally conservative decisions… and if they conducted multiple trials sooner, while the SP was being attacked, the float would be 3-4b vs 1.7. Once approved I believe other solid tumor indications will happen rapidly, not years. Heck, with their real world data, initial RA approval of ‘tumor agnostic’ is still in play IMO
Hive mind in full force today without one reply. Is it next Friday yet?
Ok DavidW2. You know better than NWBO that PR they expect RFI.
Do you think other bio company products that required RFI havent been used during the past???
I am betting on no RFI by the way. dcvax-l has been used for many years during the past. There is no safety issue at all.
But RFI never issued, need to wait 150 days to see RFI?
Not destroy it just make it so it doesn't destroy retail. Something you just don't want to understand.
Could also be that all your DCVAX hype and negativity towards TTF, influenced his decision??
“210 day with (including 60 day) RFI* - August 1st”
* If RFI was issued.
All in due time for us.
150 days + They expect RFI.
RFI around 60 days, but as other have said, it usually takes longer with NWBO.
(complex drug, no precedent as per NWBO own word, not many employee like big pharma, etc...)
Hopefully once July pass, and there is no news of approval, youll believe us.
Nothing wrong with being Aug Sep btw, only wrong when you have paid basher trying to pass as "BEARS" making predictions for "next week" , "next week", "next week", etc...
These paid basher know this. There is a team of them.
Because 150 days is made up of "clock-on time". Theoretically, if no RFI is required, the application could be decided on within 150 days.
However, RFIs are very common, and the company themselves noted (in the same PR you're referencing) that they expect an intensive period of question/answer/inspections etc.
The standard RFI is 60 "clock-off" days.
150+60=210 days from validation.
August-September.
Because EVERYTHING with NWBO always takes longer.....
What near future, if they were smart they would have started these trials ages ago. I’ve been invested for ~9 years with the initial
hope these additional trials would be initiated. Ive tempered my expectations and will be happy with a modest buy out.
A lot of the longs don’t understand the cell therapy landscape.
Please education me why Aug-Sept. timeframe.
Company requested 150 days pathway back in Dec 21 last year. 150 days is 5/24. Why needs to be Aug-Sept?
No real company can be destroyed by a message board hahahahaha
….And we have people here (working on behalf of others, all of them for money) all trying to destroy this company, which is trying to treat/cure cancer…
georgebailey,
Right now DCs are being activated and matured optimally by NWBO and T-cells are being improved by RevImmune. By combining the two the immune response can be better activated to provide more complete responses to immunotherapy. The idea for now is about combining DCVax-L with activated and amplified T-cell populations that are supercharged then educated by DCs. Sounds good to me; ). Best wishes.
Not sure if this has been posted (by Lykiri) before of not:
https://www.gofundme.com/f/glioblastoma-dcvaxl-immunotherapy-vaccine
April 17th, 2024
by Matthew Collins, Organizer
"I eat too much to die, and not enough to stay alive; I’m sitting in the middle, waiting."
Hi all,
I haven’t updated in a while. I’ve been coming to terms with my recent scan, which showed new growth in a different location in my brain. The team is unsure whether a second operation is possible as it’s much deeper in my brain than the previous tumour, but I’m having another scan on 30 April to see if the latest chemo is working, plus give a chance for the DcVax to do its thing. I’ve had my fourth dose, which, coupled with the additional hospital fees, shipping and consultation costs, has now wiped out my fundraiser. In addition, I’m having oncothermia treatment with Dr Paul Mulholland, which I have alongside my chemo. It’s £1000 session, and I’ll need to have 20+ sessions for it to be effective.
The National Cancer Research Institute (NCRI) recently reported that, despite being the biggest cancer killer of children and young adults under the age of 40, spending on brain tumour research represents just 1% of the total cancer spend. This sucks on multiple levels, not just denying young people life-extending treatment options, but knowing that there are cancer drugs out there that could potentially benefit me, but aren’t available on the NHS because they’ve not been through trials for brain cancer and therefore lack ‘evidence’ — meaning that if I want to access these drugs, I have to do a lot of the digging myself and then stump up the extortionate costs. My consultant can’t — and probably isn’t allowed under their license to practice — prescribe them to me.
I’ve paid tax my entire life, yet when I need to access treatments that could extend my life, I have to pay, and at a premium. There’s a two-tier system developing in this country: those that can afford private healthcare, and the poor sods who have to rely on the crumbs of the NHS.
Pembrolizumab, licensed for lung cancer, is a type of immunotherapy vaccine — which has shown promise in treating glioblastoma — would cost me £30,000 for a single dose.
As well as fundraising for treatments, I’ve decided to radically change what I eat, to attack the cancer through diet.
When I was diagnosed I asked about diet. The Registrar who I saw said to ‘eat what you want’. I got the impression she wanted to tag on ‘while you still can’ at the end of her sentence. So I did. Let me tell you folks, that is BAD ADVICE. Everything I’ve read since my tumour recurred has pointed to a plant-based diet, cutting out sugar and refined carbohydrates as improving outcomes for cancer patients. So I’ve made these changes, and do you know what, that shit is expensive, not to mention time-consuming. It’s a privilege to eat healthy; our Western society is fuelled on cheap, convenience foods. If you don’t have the time because you’re busy or you simply can’t afford healthy ingredients, you’re stuffed (figuratively, not literally).
When I tot up the costs of off-label drugs (antivirals and metabolic drugs that may help), supplements and therapies I’m currently taking, my spending is running at more than £2,000 per month, which far exceeds the £700 I get from Universal Credit for having a terminal illness. This is unsustainable.
I’m waiting until my next scan to decide whether to pursue a fifth dose of DcVax — I’d need to go through apheresis again, which costs £10,000 in itself, plus the vaccine costs of £25,000, consultant fees and shipping (£3,000). If the tumour has grown then I’ll see about going down a different immune therapy route — there are ‘high-risk, high-reward’ options like CAR-T cell therapy, but surprise surprise, no trials in this country, so fuck knows how I get access. I’m willing to roll the dice with any high-risk treatment at this stage, I just need to be pointed towards a trial somewhere in the world.
I’m heading down to Velindre this afternoon for some clinical psychology. I’m coping better mentally than I expected but I’m starting to resent how dismissive the stroke consultant was of me at Prince Charles Hospital back in the summer. I’ve since learned from an actual expert that if I’d suffered a brain haemorrhage as large as I did, then I’d likely not be alive. So why the effin’ fuck, given that all my vital observations were perfect, did the consultant not think I warranted further investigation? I lost two months because of that man and I don’t know if that’s what’s going to cost me my life. He and the healthcare assistant who had a go at me for leaving some clothes in the bathroom (I couldn’t walk or use my left arm) can go swivel. I will haunt you. So yeah, probably going to be helpful to vent my frustration to a mind person, get a few things off my chest.
Speaking of which, I gained loads of weight since being on steroids, but now it’s starting to fall off me and I’m caught in the crossfire between wanting to starve the cancer but not starve myself of nutrients and things that are good for the healthy parts of me. Is it possible to do a keto AND vegan diet simultaneously?
Stay beautiful,
Matt x
Did NWBO ever mention getting this nod?
>>10. Extensive amendments to a trial protocol
Sponsors are encouraged to contact the MHRA Clinical Trials Unit for advice if they plan to revise their approved protocol to such an extent that it may be more appropriate to submit an application for a new trial; for example, if the trial population, primary objectives or research hypothesis changes or if new IMPs are planned to be added to the study.
StonkMaster,
Yes, I noticed the bears were quiet before when GermanCol announced his move and both bears and some longs seem to be very quiet today after this move was justified by FDA approval and price action in this ticker. Best wishes.
|
Followers
|
1618
|
Posters
|
|
|
Posts (Today)
|
3
|
Posts (Total)
|
687472
|
|
Created
|
02/02/05
|
Type
|
Free
|
| Moderators XenaLives sentiment_stocks CaptainObvious Poor Man - Doc logic JerryCampbell | |||
![]()
“Now this is not the end. It is not even the beginning of the end. But it is, perhaps, the end of the beginning.”
~ Winston Churchill

Stylized Dendritic Cell featured on NWBO board since 2015

- Dr. Linda Liau, PhD, MBA, Professor and Chair, Department of Neurosurgery, David Geffen School of Medicine at UCLA
Clinical Trials
DCVax®-L to Treat Newly Diagnosed GBM Brain Cancer (NCT00045968) - Phase III (Double Blind)
UK (MHRA): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
DE (Germany - PEI): DCVax-L to Treat Newly Diagnosed GBM Brain Cancer (EudraCT#) 2011-001977-13
Expanded Access Protocol for GBM Patients with Already Manufactured DCVax®-L Who Have Screen-Failed Protocol 020221 (NCT02146066) (Expanded Access)
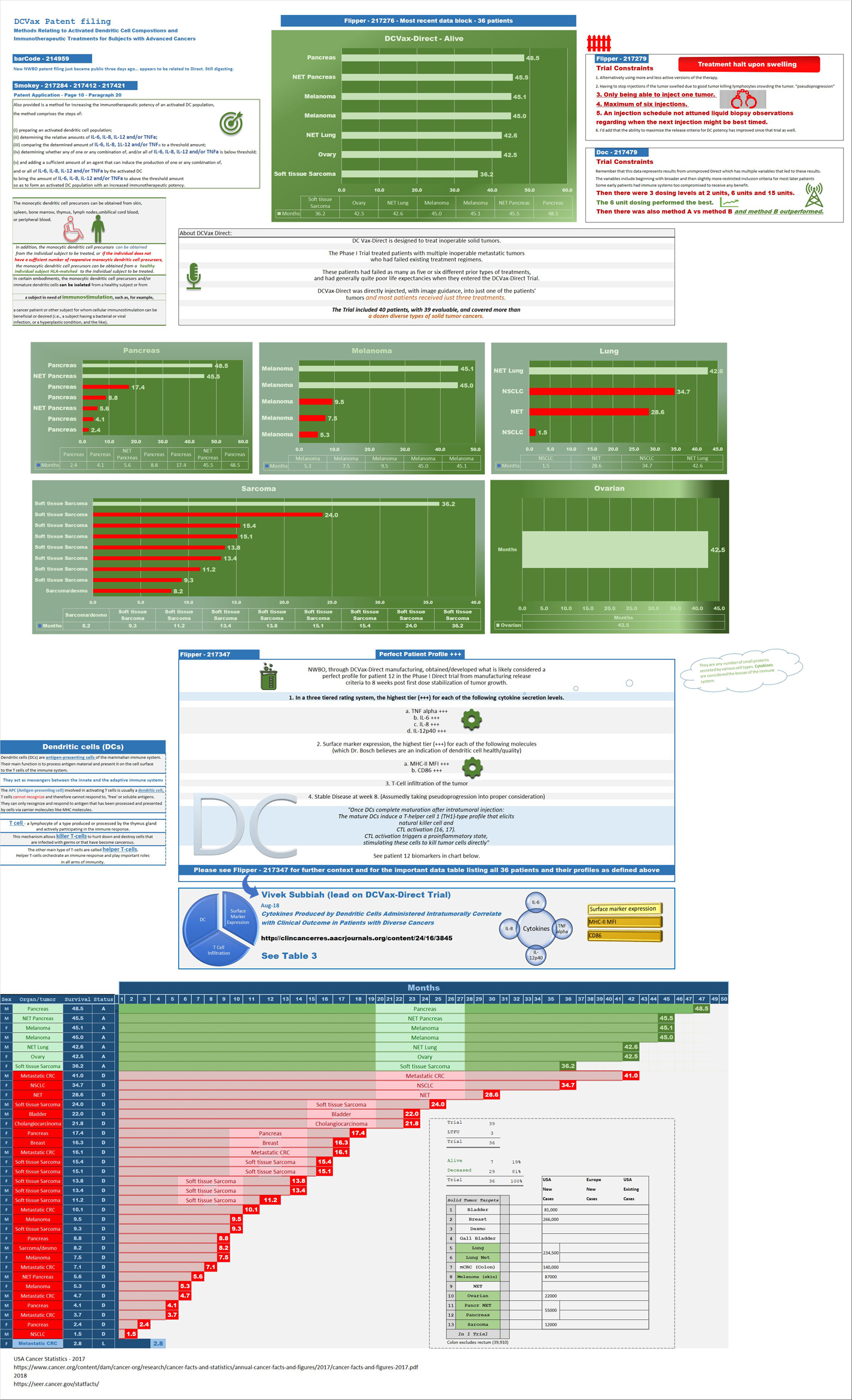
Safety and Efficacy Study of DCVax-Direct in Solid Tumors (NCT01882946) - Phase I/Phase II (Open Label)
UK Clinical Trials - Study of a Drug (DCVax®-L) to Treat Newly Diagnosed GBM Brain Cancer
EU Clinical Trials for DCVax-L - Phase III
Dendritic Cell Vaccine for Patients with Brain Tumors (NCT01204684) - Phase II - at UCLA - Randomized (Open Label) testing DCVaccine with Resiquimod and DC Vaccination with Adjuvant polyICLC
Pembrolizumab and a Vaccine (ATL-DC) for the treatment of Surgically Accessible Recurrent Glioblastoma - Phase 1 (NCT04201873)
Dendritic Cell-Autologous Lung Tumor Vaccine (DCVax-L) and Nivolumab in Treating Patients with Recurrent Glioblastoma - Phase 2 (NCT03014804)
Dendritic Cell Therapy for Brain Metastases From Breast or Lung Cancer (NCT0368765) - Phase 1 - Collaborator: Mayo Clinic
Announcement of DCVax-L and Anti-PD-1 Monoclonal Antibody (Pembrolizumab) for Patients with Liver Metastases of Primary Colorectal Carcinoma Phase 2 Trial - November 17, 2016 - University Medical Center (UMC) of the Johannes Gutenberg University of Mainz
Cognate Bioservices - Owned by Charles River Labs
Website
Company Contact Info
Investor Relations:
Les Goldman (Company) (202) 841-7909 lgoldman@nwbio.com
Sign up for Northwest email list here (hit the subscribe to email list button in the lower right)
Company Headquarters
4800 Montgomery Lane, Suite 800, Bethesda, MD 20814 (240) 497-9024
NW Bio is developing cancer vaccines designed to treat a broad range of solid tumor cancers more effectively than current treatments, and without the side effects of chemotherapy drugs. NW Bio’s proprietary manufacturing technology enables them to produce its personalized vaccine in an efficient, cost-effective manner. NW Bio has a broad platform technology for DCVax dendritic cell-based vaccines.
Their lead product, DCVax-L, is currently in a 331-patient Phase III trial for patients with newly diagnosed Glioblastoma multiforme (GBM), the most aggressive and lethal brain cancer. This trial is currently underway at 69 locations thoughout the United States, Germany and the United Kingdom. NW Bio has also conducted a Phase I/II trial with DCVax-L for late stage ovarian cancer together with the University of Pennsylvania.
Their second product, DCVax-Direct, is currently in a 60-patient Phase I/II trial for direct injection into all types of inoperable solid tumor cancers, with trials currently being conducted at both MD Anderson Cancer Center in Texas, as well as Orlando Health in Florida.
They previously received clearance from the FDA for a 612-patient Phase III trial with its third product, DCVax-Prostate, for late stage prostate cancer.
DCVAX Survival Stories & Testimonials
Alice - Metastic Merkel Cell patient from Florida - ASCO 2018
Brad Silver - GBM patient from Huntington Beach, California - ASCO 2018
Sarah Rigby - GBM patient from Hong Kong - ASCO 2018
Kristyn Power - daughter of GBM patient from Canada - ASCO 2018
Kat Charles - GBM patients from UK - ASCO 2018 - as related by her husband Jason (Kat's Cure)
Prospective patients may contact NW Bio at patients@nwbio.com
UCLA Jamil Newirth DCVax-Patient Video - 2015
Allan Butler Video - National Geographic Vice President - DCVax-Direct patient from Phase 1 Trial with Pancreatic Cancer
NWBO - Patients Sunday Dennis and Jami Newirth - Enrolled at UCLA - Vimeo, Uploaded approx. May 2015
NWBO - Vaccine Helps Keep Brain Cancer Patient Alive (Jennifer Sugioka) - NBC Channel 4, Southern California, February 24, 2015
NWBO - National Geographic's Allan Butler Stage IV Pancreatic Patient using DCVax-Direct at MD Anderson
NWBO GBM Brain Cancer Survival Story of Mark Pace

Presentations

UCLA Agreements
Prostrate
DCVax-Phase II
DCVax-Booster
Upcoming Events
Videos
Linda M. Liau, MD, PhD, MBA - April 24, 2019 at University of Washington, Neurosciences Institute
| Volume | |
| Day Range: | |
| Bid Price | |
| Ask Price | |
| Last Trade Time: |






